Default Category
-
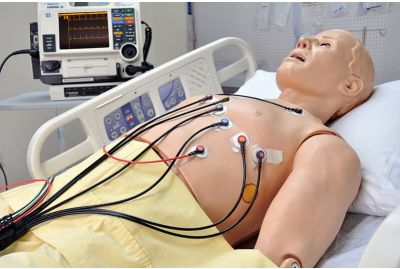 HAL® S1020 - 12-Lead ECG Skills TrainerS1020.PKLearn MoreThe HAL® S1020 is a 12-lead ECG skill trainer with an integrated myocardial infarction (MI) model to help participants improve diagnostic skills and ECG interpretation skills.
HAL® S1020 - 12-Lead ECG Skills TrainerS1020.PKLearn MoreThe HAL® S1020 is a 12-lead ECG skill trainer with an integrated myocardial infarction (MI) model to help participants improve diagnostic skills and ECG interpretation skills. -
 HAL® S1030 - Dynamic Airway and Lung Compliance SimulatorS1030.PKLearn MoreHAL® S1030 is a full-body, computer-controlled patient simulator designed for training respiratory care students and professionals on the treatment and management of respiratory diseases using a real mechanical ventilator. Just like a real patient, HAL® features a lifelike airway, can hold PEEP from 5 to 25 cmH2O, trigger the vent’s breath assist, change lung compliance and bilateral bronchial airway resistance, exhale real CO2, and much more. Together, these features allow educators to simulate diseases and conditions such as ARDS, COPD, and asthma, as seen in real life.
HAL® S1030 - Dynamic Airway and Lung Compliance SimulatorS1030.PKLearn MoreHAL® S1030 is a full-body, computer-controlled patient simulator designed for training respiratory care students and professionals on the treatment and management of respiratory diseases using a real mechanical ventilator. Just like a real patient, HAL® features a lifelike airway, can hold PEEP from 5 to 25 cmH2O, trigger the vent’s breath assist, change lung compliance and bilateral bronchial airway resistance, exhale real CO2, and much more. Together, these features allow educators to simulate diseases and conditions such as ARDS, COPD, and asthma, as seen in real life. -
 HAL® S3000 - Wireless and Tetherless, Prehospital and Nursing Care Patient SimulatorS3000.PKLearn More
HAL® S3000 - Wireless and Tetherless, Prehospital and Nursing Care Patient SimulatorS3000.PKLearn MoreHAL's advanced design and tetherless technology eliminate external tubes, wires, and compressors. HAL operates continuously during transport so that training can occur in the working environment. Rush HAL from the accident scene to the ER or the ICU while care providers diagnose and treat his condition using real monitoring and resuscitation equipment. HAL® smoothly transitions between physiologic states in response to commands from a wireless PC.
-
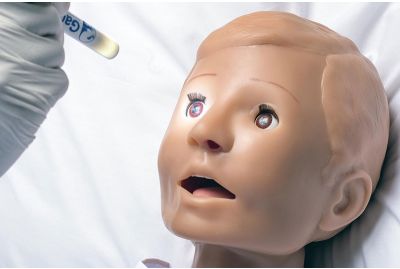
 Pediatric HAL® S3004 - Wireless and Tetherless, One-Year-Old Patient SimulatorS3004.PKLearn More
Pediatric HAL® S3004 - Wireless and Tetherless, One-Year-Old Patient SimulatorS3004.PKLearn MorePediatric HAL® is a high-fidelity toddler patient simulator specifically designed to meet the needs of pediatric care training programs. Pediatric HAL can help your care teams improve teamwork and patient care through hands-on scenario-based training. Participants can practice and develop airway management, auscultation, ventilation, CPR, IV/IO placement skills, and more.
-
 Pediatric HAL® S3005 - Wireless and Tetherless, Five-Year-Old Patient SimulatorS3005.PKLearn MoreFrom nursing to emergency care, the Pediatric HAL® S3005 Five-Year-Old Patient Simulator allows you to train teamwork and patient care skills through hands-on exercises. Pediatric HAL® is wireless and tetherless and remains fully functional while being moved from place to place.
Pediatric HAL® S3005 - Wireless and Tetherless, Five-Year-Old Patient SimulatorS3005.PKLearn MoreFrom nursing to emergency care, the Pediatric HAL® S3005 Five-Year-Old Patient Simulator allows you to train teamwork and patient care skills through hands-on exercises. Pediatric HAL® is wireless and tetherless and remains fully functional while being moved from place to place. -
 Newborn HAL® S3010 - Wireless and Tetherless, Neonate at 40-Weeks Gestational AgeS3010.PKLearn More
Newborn HAL® S3010 - Wireless and Tetherless, Neonate at 40-Weeks Gestational AgeS3010.PKLearn MoreNewborn HAL's® true-to-life physical and physiological features, wireless mobility, and ease-of-use allow you to simulate realistic clinical cases. Whether training occurs in a simulation center, in situ, or in transit, participants of any level can practice the skills needed to provide safe and effective care to neonatal patients.
-
 Replacement Trachea Skin for Trauma HAL® S3040.100 - Set of 10 (S3040.100.122)13080372ALearn MoreThe Trauma HAL® S3040.100 manikin has many lifelike airway features that allow participants to use real equipment and hone surgical airway procedures like a tracheostomy. This is a set of ten replacement trachea skins for the Trauma HAL® S304.100 manikin that allows participants to practice tracheostomy skills and ensure clinical competence.
Replacement Trachea Skin for Trauma HAL® S3040.100 - Set of 10 (S3040.100.122)13080372ALearn MoreThe Trauma HAL® S3040.100 manikin has many lifelike airway features that allow participants to use real equipment and hone surgical airway procedures like a tracheostomy. This is a set of ten replacement trachea skins for the Trauma HAL® S304.100 manikin that allows participants to practice tracheostomy skills and ensure clinical competence. -
 Replacement Cricothyroid Membranes for Trauma HAL® S3040.100 - Set of 10 (S3040.100.037.R2)11160225ALearn MoreThe Trauma HAL® S3040.100 manikin has many lifelike airway features that allow participants to use real equipment and practice surgical airway procedures like a cricothyrotomy. This is a set of ten replacement cricothyroid membranes for the Trauma HAL® S304.100 manikin that helps participants practice this procedure and ensure clinical competence.
Replacement Cricothyroid Membranes for Trauma HAL® S3040.100 - Set of 10 (S3040.100.037.R2)11160225ALearn MoreThe Trauma HAL® S3040.100 manikin has many lifelike airway features that allow participants to use real equipment and practice surgical airway procedures like a cricothyrotomy. This is a set of ten replacement cricothyroid membranes for the Trauma HAL® S304.100 manikin that helps participants practice this procedure and ensure clinical competence. -
 HAL® S315.100 - Adult Multipurpose Airway and CPR TrainerS315.100.M2.PKLearn MoreHAL® S315.100 is an easy-to-use and portable airway management and CPR skills trainer. HAL was designed to help you teach basic and advanced airway management as well as cardiopulmonary resuscitation. HAL helps participants learn to recognize laryngospasm and practice performing emergency tracheostomies and cricothyrotomies. HAL® is available in a full-body configuration.
HAL® S315.100 - Adult Multipurpose Airway and CPR TrainerS315.100.M2.PKLearn MoreHAL® S315.100 is an easy-to-use and portable airway management and CPR skills trainer. HAL was designed to help you teach basic and advanced airway management as well as cardiopulmonary resuscitation. HAL helps participants learn to recognize laryngospasm and practice performing emergency tracheostomies and cricothyrotomies. HAL® is available in a full-body configuration. -
 HAL® S315.200 - Adult Heart and Lung Sounds Skills TrainersS315.200.M2.PKLearn MoreThe HAL® S315.200 is a Gaumard® manikin designed to help teach site-specific heart and lung auscultation skills using seamless simulation technology. Simply press the bell against the skin and listen. The students use realistic and palpable anatomic landmarks on the manikin to locate the site where a specific sound should be heard. If correct, they will hear the appropriate sound through the stethoscope and/or external speakers.
HAL® S315.200 - Adult Heart and Lung Sounds Skills TrainersS315.200.M2.PKLearn MoreThe HAL® S315.200 is a Gaumard® manikin designed to help teach site-specific heart and lung auscultation skills using seamless simulation technology. Simply press the bell against the skin and listen. The students use realistic and palpable anatomic landmarks on the manikin to locate the site where a specific sound should be heard. If correct, they will hear the appropriate sound through the stethoscope and/or external speakers.